Last updated: May 2026
This guide covers upper arm, forearm, and neurovascular anatomy for students, fitness trainees, and curious readers. It does NOT address hand or wrist anatomy in depth those deserve their own breakdown.
Arm Anatomy: Every Bone, Muscle and Nerve Actually Explained
Most arm anatomy guides do one of two things. They go so deep into Latin nomenclature that you need a medical dictionary to read them, or they stay so surface level that you leave knowing only “biceps = front, triceps = back.” Neither is useful. This guide sits between both.
What Is Arm Anatomy? (And Why the Definition Matters)
Arm anatomy refers to the study of the structural components of the upper extremity including bones, muscles, nerves, and blood vessels that work together to produce movement, force, and sensation from the shoulder to the fingertips.
Here’s the thing: technically, the “arm” in anatomical terms means only the segment between the shoulder joint and the elbow. The section from elbow to wrist is the forearm. Most people use arm to describe the whole limb. Both usages are fine in casual conversation, but in any clinical or training context, the distinction changes everything about where you’re talking about.
Arm anatomy is the study of the bones, muscles, nerves, and vessels that make up the upper extremity. It spans from the shoulder joint to the fingertips and contains 30 bones total, innervated by the brachial plexus (C5–T1).
The Bones: The Framework Everything Else Hangs From
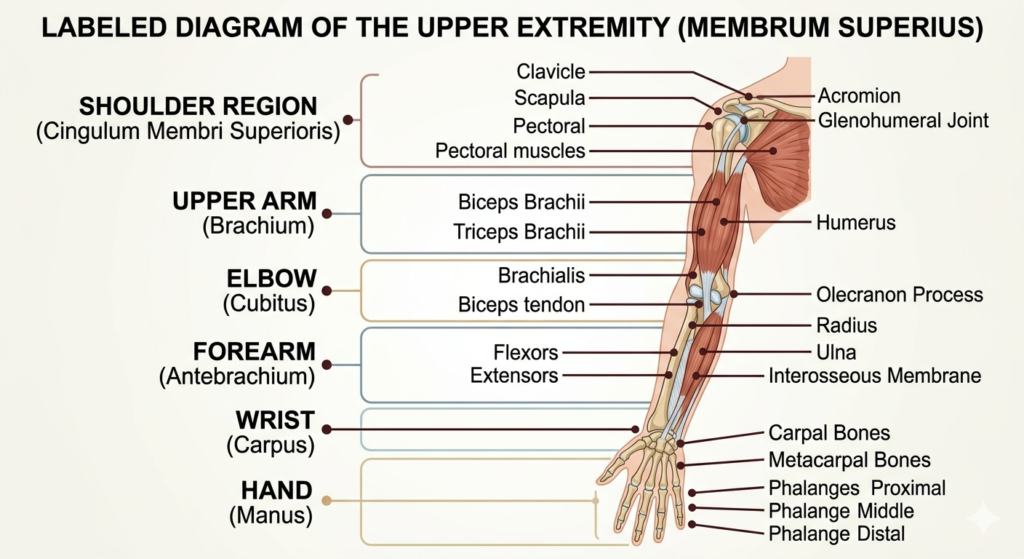
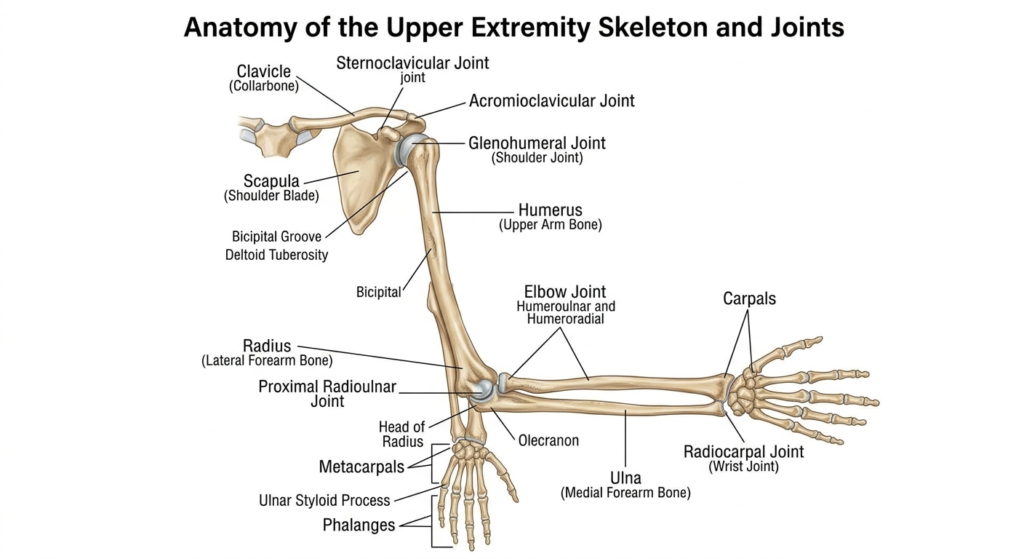
The entire upper extremity is built on 30 bones. That includes the shoulder girdle, the upper arm, the forearm, the wrist, and the hand.
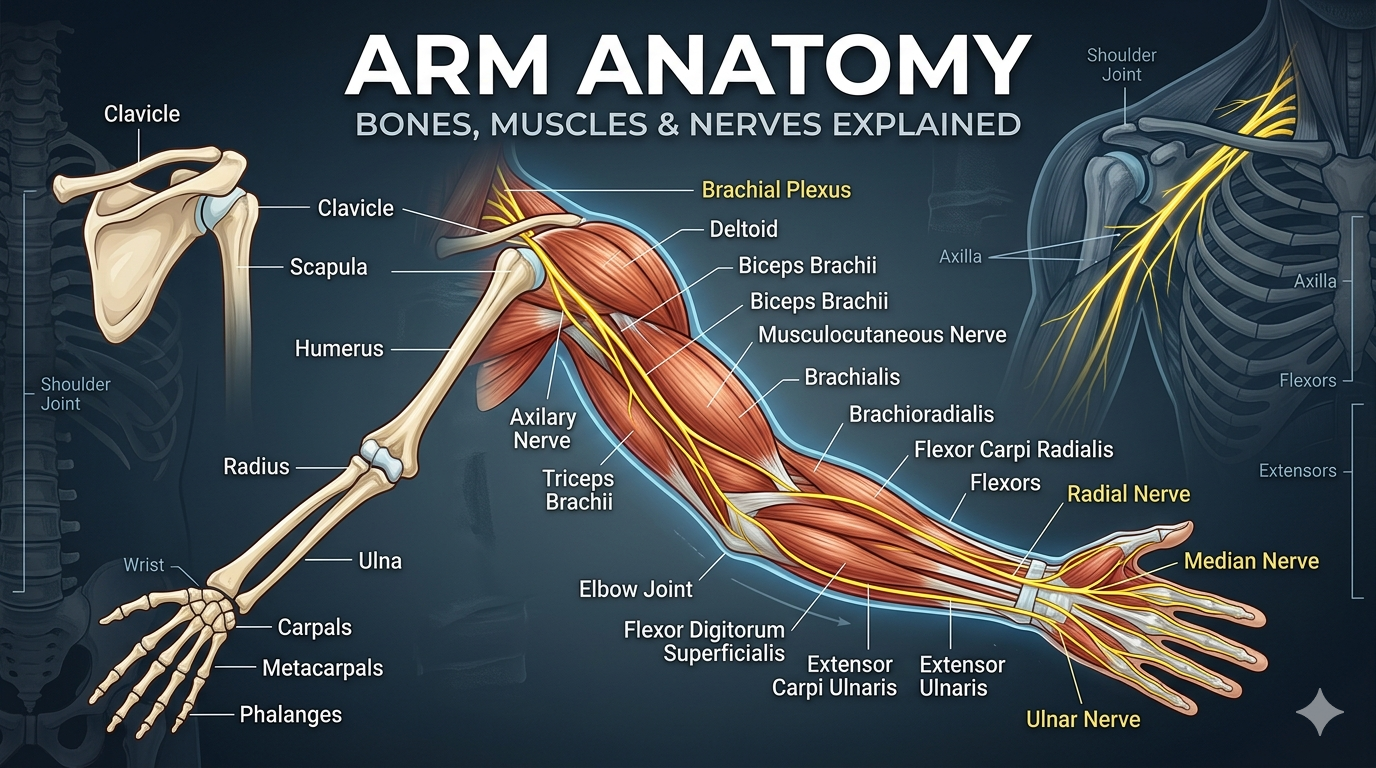
For students and trainers, the three bones you’ll encounter most are the humerus, radius, and ulna.
The humerus is the single long bone of the upper arm. It connects to the scapula at the glenohumeral joint a ball and socket design that sacrifices stability for mobility. This is why shoulder dislocations are so much more common than hip dislocations; the socket is considerably shallower.
The radius and ulna form the forearm. When your palm faces forward (the standard anatomical position), the radius is on the thumb side, the ulna on the pinky side. What makes them unique is that the radius can rotate around the ulna that’s what allows you to turn your palm up (supination) and palm down (pronation).
The scapula and clavicle complete the shoulder girdle. They act as the bridge between the arm and the axial skeleton, distributing forces across the torso rather than concentrating them in a single joint.
Upper Arm Muscles: Anterior vs. Posterior Get This Right Once
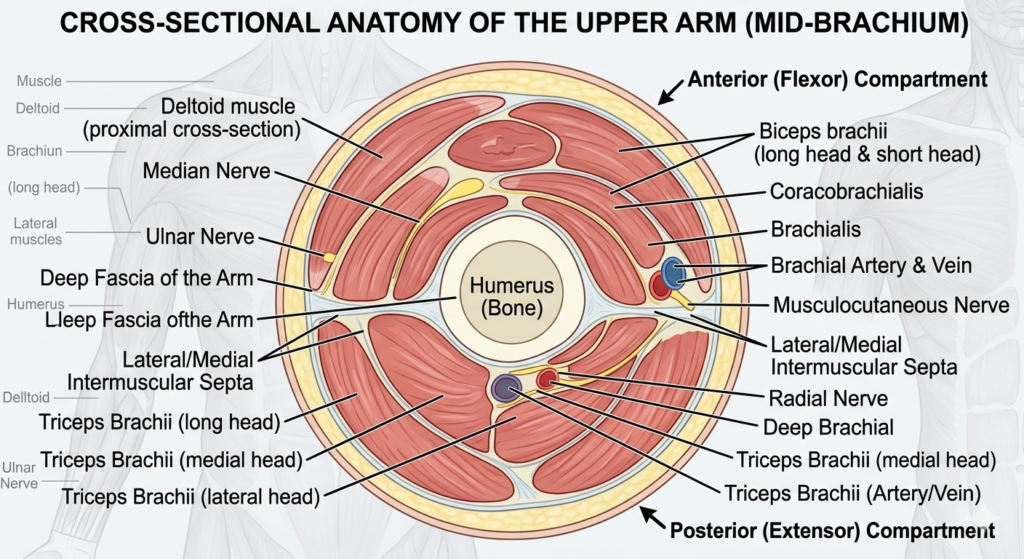
This is where most students get tripped up. The muscles of the upper arm are divided into two compartments by fibrous walls (intermuscular septa) that attach to the humerus. Front compartment = flexors. Back compartment = extensors.
Anterior (flexor) compartment contains three muscles:
The biceps brachii has two heads a long head from the supraglenoid tubercle of the scapula, a short head from the coracoid process. It’s the most recognizable muscle in the body. What most guides skip is that the biceps actually has three functions: elbow flexion, forearm supination, and minor stabilization of the glenohumeral joint. Targeting all three in training requires varied hand positions, not just curls.
The brachialis sits deep to the biceps and is often called the “true” elbow flexor because unlike the biceps, it only flexes the elbow no supination role at all. It’s the strongest elbow flexor. Students consistently underestimate it because it’s invisible under the biceps.
The coracobrachialis is the smallest of the three. It mainly flexes and adducts the arm at the shoulder. It doesn’t cross the elbow. Most anatomy textbooks mention it briefly and move on; most gym goers have never heard of it.
Posterior (extensor) compartment contains just one muscle:
The triceps brachii has three heads long, medial, and lateral. It’s the primary extensor of the elbow and the largest muscle in the arm by volume, a fact that surprises people who spend all their time curling. If your goal is bigger looking arms, triceps training gives more return per set than biceps training. That’s an opinion many will push back on, but the volume math supports it.
Forearm Muscles 20 Muscles in Two Compartments
Or maybe I should say it this way the forearm is where arm anatomy gets genuinely hard, and where most guides give up and just list names.
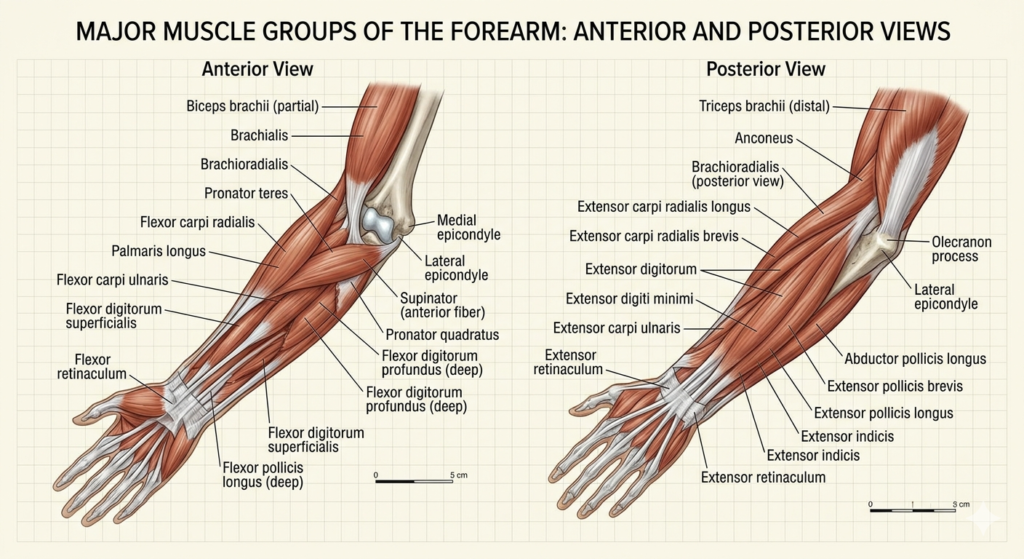
There are 20 muscles in the forearm, split into anterior (flexor) and posterior (extensor) compartments. They’re further organized into superficial, intermediate, and deep layers.
The anterior group controls wrist and finger flexion, plus forearm pronation. Key muscles include flexor carpi radialis, flexor carpi ulnaris, and flexor digitorum superficialis. The posterior group controls wrist and finger extension plus supination extensor carpi radialis longus and brevis, extensor digitorum, and the supinator being the most clinically relevant.
The brachioradialis gets its own mention because it’s anatomically in the posterior compartment but functions as an elbow flexor. It’s strongest when the forearm is in a neutral (thumb up) position. Hammer curls preferentially load it.
Quick note: For exam purposes, knowing which nerve innervates which compartment is more testable than memorizing every muscle name. More on that in the next section.
The Nerves: Brachial Plexus and Why It Matters
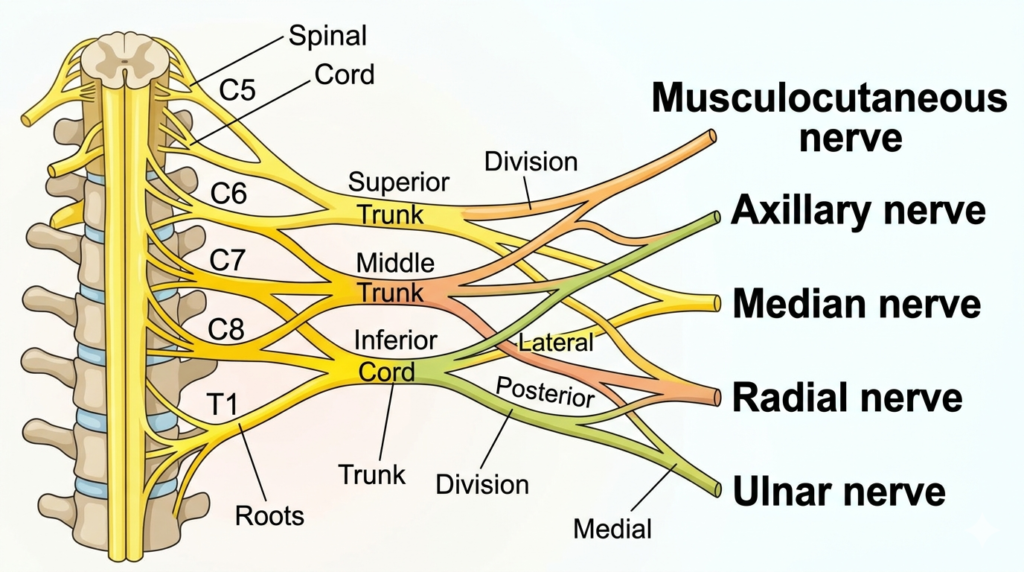
Every single structure in the upper extremity is innervated by the brachial plexus a network of nerves originating from spinal roots C5 through T1. According to StatPearls (NCBI, updated 2023), understanding nerve to bone relationships is critical in clinical settings: injuries at different points along the humerus predictably damage different nerves.
The mnemonic “ARM” is worth knowing:
A Axillary nerve (C5–C6): damaged in neck of humerus fractures. Result: deltoid weakness, loss of sensation over the shoulder.
R Radial nerve (C5–T1): damaged in midshaft humerus fractures. Result: wrist drop inability to extend the wrist. This is one of the more dramatic neurological signs in orthopedic emergencies.
M Median nerve (C6–T1): damaged in supracondylar fractures (common in children). Result: loss of thumb opposition, “hand of benediction” when attempting to make a fist.
The musculocutaneous nerve (C5–C7) innervates the entire anterior compartment of the upper arm all three muscles and then becomes the lateral cutaneous nerve of the forearm, providing sensation to the outer forearm. The radial nerve handles the posterior compartment.
I’ve seen conflicting breakdowns of which nerve roots contribute to specific muscles across different anatomy texts Gray’s Anatomy and StatPearls occasionally vary by a root level. The clinical mnemonic “ARM” is universally agreed upon, but for precise academic citing, StatPearls (2023) is the more current reference.
Blood Supply: The Brachial Artery and Its Branches
The brachial artery is the main arterial supply to the arm. It begins at the lower border of teres major (where the axillary artery becomes the brachial artery) and runs along the medial side of the arm, between the biceps and triceps muscles.
In the cubital fossa at the elbow, the brachial artery divides into the radial and ulnar arteries the two main vessels of the forearm.
Clinically, the brachial artery is where blood pressure is measured. The median cubital vein in the cubital fossa is where blood draws are performed it connects the cephalic and basilic veins superficially and is usually the most accessible large vein in the body.
Upper Arm vs. Forearm: A Quick Comparison
Quick Comparison
| Structure | Upper Arm | Forearm |
|---|---|---|
| Bones | Humerus (1) | Radius + Ulna (2) |
| Muscle count | 4 (+ rotator cuff nearby) | 20 |
| Primary nerve | Musculocutaneous + Radial | Median + Ulnar + Radial |
| Main artery | Brachial | Radial + Ulnar |
| Key joint | Elbow (hinge + pivot) | Proximal radioulnar (rotation) |
The upper arm is simpler in structure but carries higher clinical stakes. The forearm is more complex but its injuries are generally less neurologically dangerous.
Clinical Relevance: What Anatomy Means When Things Go Wrong
Most anatomy guides teach you where things are. Fewer explain what breaks when.
Wrist drop a midshaft humerus fracture compresses the radial nerve in the spiral groove. The patient can’t extend the wrist or fingers. The diagnosis is almost certain from the mechanism alone before imaging confirms it.
Popeye sign rupture of the long head of the biceps tendon causes the muscle belly to bunch up into a visible ball on flexion. According to TeachMeAnatomy (2026), patients actually retain most elbow flexion strength because the brachialis and supinator compensate. The aesthetic deformity is worse than the functional loss.
Bicipital aponeurosis an often ignored fibrous band that fans from the biceps tendon across the cubital fossa. In IV placement, it lies directly over the brachial artery. Nurses and phlebotomists locate veins by feel in this region; knowing the aponeurosis is there explains why palpation in the cubital fossa is technique dependent.
Look if you’re studying for an OSCE or a clinical anatomy practical, here’s what actually works: learn the fracture to nerve relationships first (the ARM mnemonic), then build the muscle to nerve table, then add blood supply last. Most clinical questions test the first two, rarely the third.
Arm Anatomy for Fitness: Mapping Muscles to Training
Some experts argue that training specificity matters more than anatomical knowledge. That’s valid if you’re following a well designed program someone else built. But if you’re troubleshooting a plateau, an imbalance, or a persistent ache, knowing what you’re actually loading changes everything.
Anterior compartment training: Supinated curls bias the biceps (especially supination function). Neutral grip hammer curls shift load to the brachioradialis. Incline curls put the long head under a greater stretch. Most people undertrain the brachialis it responds best to elbow flexion under load regardless of grip, and adding direct brachialis work is one of the fastest ways to increase upper arm girth.
Posterior compartment training: Overhead triceps extensions load the long head most because it crosses the shoulder joint. Pushdowns bias the lateral and medial heads. If you only do one triceps movement, the overhead extension gives the most complete stimulus.
Forearm training: Wrist curls for the flexors, reverse curls for the extensors. Neglecting extensors relative to flexors is one of the more common contributors to medial elbow discomfort in lifters.
Note: This is general educational information, not medical or training advice. If you’re managing an existing injury, consult a physiotherapist or sports medicine physician before loading these structures.