Why Your “Just Stress” Has a Clinical Name And What Women’s Mental Health Month Was Built to Say
Women’s mental health month refers to a designated awareness period observed in May alongside National Mental Health Month, and in March by advocacy organizations including Contigo Wellness that spotlights mental health conditions disproportionately affecting women. It exists because women face depression, anxiety, PTSD, and burnout at measurably higher rates than men, yet remain significantly undertreated.
What Women’s Mental Health Month Is and Why a General Awareness Month Wasn’t Enough
May has been National Mental Health Month in the U.S. since 1949. Women’s mental health month, as a women-specific observance, is newer and still being formalized across the advocacy landscape.
Here’s the thing: women experience depression at roughly twice the rate of men. According to NIMH data, more than 10% of women have a major depressive episode annually, compared to 6.2% of men. That gap isn’t biological inevitability. It’s shaped by hormones, caregiving load, trauma exposure, and systemic barriers to care that a gender-neutral awareness campaign simply doesn’t address.
Contigo Wellness, an Austin-based mental health nonprofit, has been pushing March as the official Women’s Mental Health Awareness Month, tying it to Women’s History Month. NAMI and major national organizations observe May. The result? Women’s mental health now gets two months of dedicated attention which, given the data, is the least it deserves.
Women’s mental health month exists because the general conversation wasn’t specific enough.
The Mental Health Conditions That Hit Women Hardest and the Data Behind Them
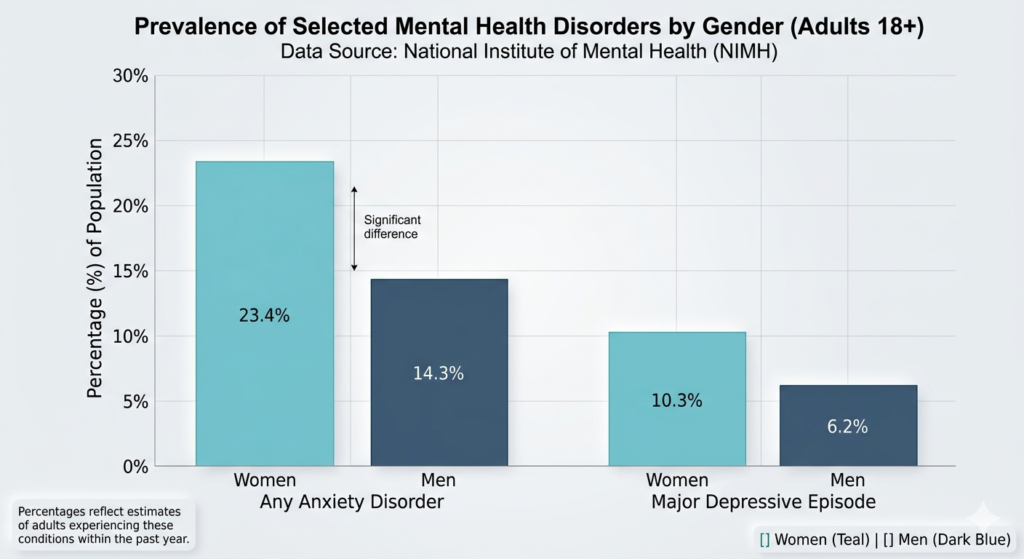
Anxiety is the most prevalent mental health condition in America. Women experience it at a rate of 23.4%, compared to 14.3% in men nearly a 10 point gap, per NIMH data compiled by The World Data, 2025. Depression follows the same pattern.
PTSD is where the data gets uncomfortable. Women develop it at twice the rate of men, despite men having higher overall exposure to traumatic events. The reason isn’t fragility it’s the type of trauma. Sexual violence and intimate partner violence, which women disproportionately experience, carry a higher PTSD conversion rate than combat trauma. That’s a finding from the Journal of Traumatic Stress, 2024–2025 research cycle.
Or maybe I should say it this way: the conditions women develop most often aren’t random. They map directly onto the specific stressors women face at higher rates than men.
Perinatal mood and anxiety disorders (PMADs) get collapsed into “postpartum depression” in most public health messaging but PMADs include prenatal depression, postpartum anxiety, and postpartum OCD. About 1 in 8 mothers develops postpartum depression, per the Office on Women’s Health. PMADs collectively affect closer to 1 in 5 pregnant and postpartum women.
Most people assume postpartum depression is the full picture. The data says otherwise postpartum anxiety is actually more common in the perinatal period than depression. It’s just discussed far less.
Hormonal Mental Health Triggers Most Articles Skip Entirely
This is the gap both competitor articles miss and it affects millions of women.
PMDD (Premenstrual Dysphoric Disorder) affects an estimated 3–8% of menstruating women. It’s frequently misdiagnosed as “bad PMS” or dismissed as emotional instability. PMDD causes severe depression, anxiety, and irritability in the luteal phase the 1–2 weeks before menstruation then clears shortly after menstruation begins. The cyclical pattern is diagnostic. It has a clinical ICD code. It responds to treatment.
Perimenopause related depression is even less talked about. Hormonal shifts in perimenopause which can begin in the mid to late 30s directly increase the risk of depression and anxiety, even in women with zero prior mental health history. The 2024 Menopause Society clinical guidelines explicitly acknowledge this link. Many women in this window get bloodwork done, get told their results are “within normal range,” and leave without an answer.
That is a systemic failure. Not a personal one.
To get appropriate care for hormonal mental health symptoms, follow these steps:
- Track mood symptoms alongside your cycle for at least two full months.
- Bring a written log not just a verbal description to your appointment.
- Ask your provider about PMDD screening using the Daily Record of Severity of Problems (DRSP) tool.
- If your GP or OB isn’t familiar with PMADs, ask for a referral to a reproductive psychiatrist.
Workplace Burnout Is a Women’s Mental Health Crisis The Numbers Are Hard to Dismiss
Look if you’ve been telling yourself your exhaustion is just a busy season, you’re not alone. But what the data shows isn’t stress. It’s structural.
According to the Mind Share Partners 2025 Mental Health at Work Report, women accounted for 71% of all mental health related workplace leaves taken in early 2024. Women are also 8 percentage points more likely than men to report feeling like they’re “struggling or in crisis” at work.
75% of women report experiencing burnout. 58% of men say the same.
Female burnout rates are up 4% year over year. Male burnout rates are down 3%.
Some experts argue this gap partly reflects women’s higher likelihood to self report mental health struggles honestly and that’s a valid point for survey data. But behavior is harder to fake than surveys. When 71% of mental health workplace leaves belong to women, the conversation has moved past self reporting bias.
The NAMI 2025 Workplace Mental Health Poll found that 46% of workers worry about losing their job if they discuss mental health at work. For women in male dominated industries, that fear often has documented precedent which creates a catch 22 where the people carrying the highest burden have the highest cost of asking for help.
How to Actually Get Support Not Just a List of Phone Numbers
Most mental health articles close with a box of hotlines and call it done. That’s not enough.
If you can’t afford therapy right now: NAMI (National Alliance on Mental Illness) runs a free peer support helpline at 1-800-950-NAMI (6264) and hosts local support groups at no cost. These aren’t crisis lines they’re ongoing peer connections, which is a different kind of support and often more sustainable long term.
If you want to try therapy but don’t know where to start: Talkspace and BetterHelp both offer sliding scale pricing with therapists who specialize in women’s issues, postpartum mental health, and reproductive psychiatry. I’ve seen conflicting data here some studies show comparable outcomes to in-person therapy for mild to moderate anxiety and depression; others show reduced effectiveness for complex trauma and PTSD. My read: app-based therapy is a strong, accessible starting point. It’s not the ceiling.
If you’re in immediate distress: SAMHSA’s National Helpline 1-800-662-4357 is free, confidential, and available 24/7. It connects callers directly to local treatment facilities and support groups. No insurance required.
What most guides skip is this: many women don’t need weekly therapy as a first step. They need psychoeducation a clear explanation of what’s actually happening in their body and brain. NAMI’s free online courses and SAMHSA’s treatment locator are among the most underused tools available, and they require no diagnosis, no referral, and no cost.
Quick Comparison: Women’s Mental Health Support Options
| Option | Best For | Key Benefit | Limitation |
|---|---|---|---|
| NAMI Helpline (free) | Ongoing peer support | No cost, community based | Not clinical therapy |
| Talkspace / BetterHelp | Affordable therapy entry point | Accessible, flexible scheduling | Less effective for complex trauma |
| SAMHSA Helpline (free) | Immediate local referrals | 24/7, no insurance needed | Referral only not direct care |
| Reproductive Psychiatrist | PMDD, perimenopause linked depression | Hormonal mental health expertise | Hard to find, often out of network |
| Local NAMI Chapters | Education + community connection | Free groups, peer led | Availability varies by region |